Inosine Pranobex is the first antiviral agent used to treat SSPE.
Subacute sclerosing panencephalitis (SSPE) is a rare, but devastating complication of the measles virus.
Inosine pranobex is the first antiviral agent used to treat SSPE.
It boosts T-cell lymphocyte proliferation, natural killer cell activity, and pro-inflammatory cytokines, restoring immunosuppressed patient’s deficient responses.
High Grade Threats
for SSPE Patients
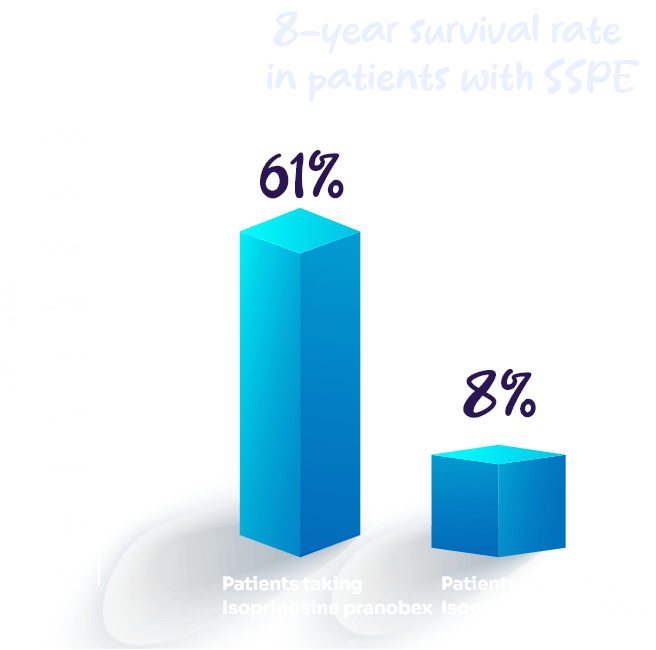
SSPE is associated with high mortality rates.
Patients with SSPE die within 1–3 years of diagnosis
In acute fulminant SSPE, patients die much earlier
Prolong your patient’s life with Inosine pranobex
Inosine pranobex has been explored as a potential treatment for SSPE, although its effectiveness in halting disease progression remains uncertain. progression of SSPE and improving certain neurological symptoms in some patients.
SSPE manifests 5 to 10 years after measles and presents with the following behavioral impairment and mental disturbances.
Myoclonia
Gait difficulties
Selective Mutism
Dementia
Autonomic disturbances
Findings of pyramidal tract involvement
Positive Results
Get your patients into remission with Inosine pranobex
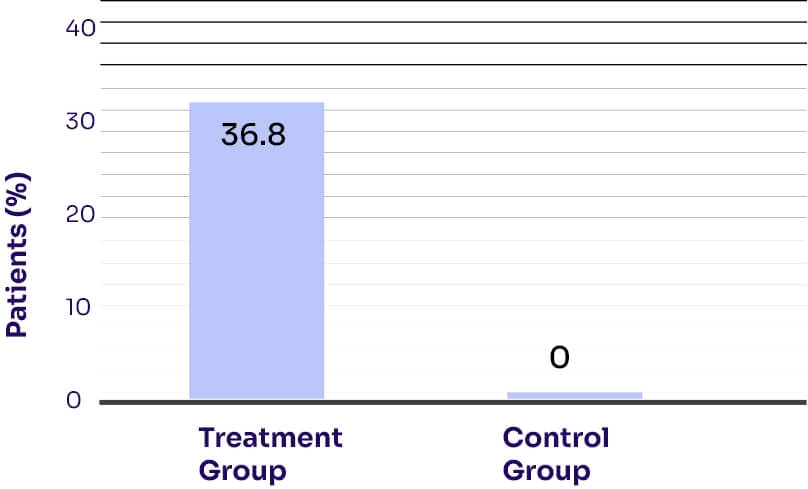
A case-control study compared patients with SSPE who received treatment consisting of Inosine pranobex 100 mg/kg/day, subcutaneous interferon α-2a 10 mU/m2/three times a week, and oral lamivudine 10 mg/kg/day (n = 19) with those who did not receive any treatment (n = 13).
The remission rates for the treatment group were significantly higher than the control group (P = 0.036).6
In 10% of cases, SSPE progresses rapidly, ultimately resulting in death.
Stabilize your patients with Inosine pranobex and improve their quality of life
Improved Results
Three studies showed stabilization and improvement with Inosine pranobex treatment in ≥ 50% SSPE patients
Inosine pranobex was administered in an open therapeutic trial involving 15 SSPE patients
Five patients experienced long- term remissions
Nine months after treatment commenced, one patient achieved remission
Three patients experienced temporary remissions or stabilization
Inosine pranobex is well tolerated for an extended period of time.
Long-term administration of Inosine pranobex in SSPE patients is safe and lacks significant adverse side effects
Indication and Important Safety Information
Isoprinosine is intended to be used for:
⮚ Severe measles ⮚ SSEP
Contraindications
Isoprinosine is contraindicated in the following:
⮚ Hypersensitivity to the drug components; ⮚ Gout; ⮚ Kidney stone disease; ⮚ Arrhythmia; ⮚ Chronic renal failure; ⮚ Children under 3 years old (body weight up to 15-20 kg)
After 2 weeks of using Isoprinosine, a concentration of uric acid in the blood serum and urine should be monitored. It is advisable to monitor liver and kidney functions (plasma transaminase activity, creatinine, uric acid) every month after a 4-week use, in case of the long-term application. It is necessary to control the level of uric acid in the blood serum when using Isoprinosine in combination with drugs that increase the level of uric acid or drugs that impair renal function.
Adults and the Elderly:
The recommended dosage is 50mg/kg – 100mg/kg of body weight usually 3g/day up to a maximum of 4g/day, administered orally in 3-4 equally divided doses during waking hours. Subacute sclerosing panencephalitis (SSPE): 50-100mg/kg daily, up to a maximum of 3-4 g, in divided doses every 4 hours, with regular monitoring to evaluate patient status and requirement for extended treatment.
The weight of the patient and the severity of the disease are important factors in determining the dosage.
Side Effects
The incidence of side effects after using the drug is classified according to WHO recommendations.10
⮚ Often: ≥1% and <10%.
⮚ Sometimes: ≥0.1% and <1%.
On the part of the gastrointestinal tract: often - nausea, vomiting, epigastric pain; sometimes - diarrhea, constipation.
On the part of the liver and biliary tract: often - a temporary increase in the activity of transaminases and alkaline phosphatase in blood plasma, an increase in the concentration of urea in blood plasma.
On the part of the skin and subcutaneous fat: often - itching.
On the part of the nervous system: often - headache, dizziness, weakness; sometimes - drowsiness, insomnia.
On the part of the urinary system: sometimes - polyuria.
On the part of the musculoskeletal system and connective tissue: often - joint pain, exacerbation of gout.
Cases of the drug overdose are not described.
Immunosuppressants may decrease the effectiveness of the drug action. Xanthine oxidase inhibitors and uricosuric agents (including diuretics) may enhance the risk of an increase of the serum uric acid level in patients taking Isoprinosine.
It is not recommended to use the drug during pregnancy and lactation, since the safety of use has not been studied.
Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis [Internet] [Updated 2023 May 19]. Available at: https://pubmed.ncbi.nlm.nih.gov/32809508/. Accessed on Nov 11, 2023.
Memon SA, Afzal SS, Tukruna A, Khan AT, Tebha SS, Zaidi ZA. Trends and Treatment of Sub-Acute Sclerosing Panencephalitis: An Updated Review. Glob Pediatr Health. 2021;8:2333794X211065330.
Sliva J, Pantzartzi CN, Votava M. Inosine Pranobex: A Key Player in the Game Against a Wide Range of Viral Infections and Non-Infectious Diseases. Adv Ther. 2019;36(8):1878–905.
Garg RK, Sharma PK, Kumar N, Pandey S. Subacute Sclerosing Panencephalitis in Older Adulthood. Tremor Other Hyperkinet Mov (N Y). 2019;9.
Jones CE, Dyken PR, Huttenlocher PR, Jabbour JT, Maxwell KW. Inosiplex therapy in subacute sclerosing panencephalitis. A multicentre, non-randomised study in 98 patients. Lancet. 1982;1(8280):1034–7.
Aydin OF, Senbil N, Kuyucu N, Gürer YK. Combined treatment with subcutaneous interferon-alpha, oral isoprinosine, and lamivudine for subacute sclerosing panencephalitis. J Child Neurol. 2003;18(2):104–8.
Gokcil Z, Odabasi Z, Demirkaya S, Eroglu E, Vural O. Alpha-interferon and isoprinosine in adult-onset subacute sclerosing panencephalitis. J Neurol Sci. 1999 Jan 1;162(1):62–4.